
Twists and Turns: Navigating Clinicoradiological Presentations, Decision Making in Management and Histopathological Revelations of Adnexal Torsion
Abstract:
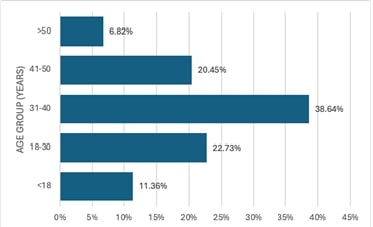
Adnexal torsion is a rare condition that can be potentially fatal if untreated. It has a varied clinical presentation and can affect any age group. Clinicians can diagnose and treat adenexal torsion more accurately if they are aware of the clinical and pathological characteristics of the patients. To analyze the clinical and pathological profile of adnexal torsion cases in Saveetha Medical College. The study was a retrospective analysis of hospital records which included all cases of adnexal torsion that underwent treatment between January 2023 to January 2024 in Saveetha Medical College. The majority (61.37%) of participants were in the reproductive age group (18-40 years). Abdominal pain was the most common symptom seen in 84.44% of patients. Majority of the women belonged to Para 2 (54.44%) and Para 1 (24.24%). Half the subjects underwent Vaginal delivery while the remaining underwent Caesarean section. A right-sided predominance was observed with most of them having one and two turns (32%). On histopathological examination, a simple serous cyst (25%) was the most predominant finding. Even though adnexal torsion is a rare clinical illness, it typically manifests as an emergency. A high degree of suspicion is necessary for the diagnosis because there are many possible clinical presentations. However, the diagnosis can only be confirmed on the operating table. The patient should be operated on as soon as possible to prevent complications and aid in conserving the ovary.References:
[1]. Warner, M.A.,
Fleischer, A.C., Edell, S.L., Thieme, G.A., Bundy, A.L., Kurtz, A.B., et al.,
1985. Uterine adnexal torsion: sonographic findings. Radiology, 154,
773–775.
[2]. Provost, R.W.,
1972. Torsion of the Normal Fallopian Tube. Obstetrics & Gynecology,
39, 80.
[3]. Bider, D.,
Mashiach, S., Dulitzky, M., Kokia, E., Lipitz, S., Ben-Rafael, Z., 1991.
Clinical, surgical and pathologic findings of adnexal torsion in pregnant and
nonpregnant women. Surg Gynecol Obstet, 173, 363–366.
[4]. Vijayalakshmi, K.,
Reddy, G.M.M., Subbiah, V.N., Sathiya. S., Arjun, B., 2014.
Clinico-pathological profile of adnexal torsion cases: a retrospective analysis
from a tertiary care teaching hospital. J Clin Diagn Res, 8, OC04-07.
[5]. Verma, M., Bhuria,
V., Chauhan, M., Nanda, S., Dahiya, P., Singhal, S.R., 2021. Adnexal torsion: a
retrospective analysis from a tertiary care teaching hospital in northern india.
Cureus, 13, e17792.
[6]. Chang, H.C.,
Bhatt. S., Dogra. V.S., 2008. Pearls and pitfalls in diagnosis of ovarian
torsion. Radio Graphics, 28, 1355–1368.
[7]. Gupta, A.,
Gadipudi, A., Nayak, D., 2020. A five-year review of ovarian torsion cases:
lessons learnt. J Obstet Gynaecol India, 70, 220–224.
[8]. Houry, D., Abbott,
J.T., 2001. Ovarian torsion: a fifteen-year review. Ann Emerg Med, 38,
156–159.
[9]. Balci, O., Icen,
M.S., Mahmoud, A.S., Capar, M., Colakoglu, M.C., 2011. Management and outcomes
of adnexal torsion: a 5-year experience. Arch Gynecol Obstet, 284,
643–646.
[10]. Mashiach, R.,
Melamed, N., Gilad, N., Ben-Shitrit, G., Meizner. I., 2011. Sonographic
diagnosis of ovarian torsion: accuracy and predictive factors. J Ultrasound
Med, 30, 1205–1210.
[11]. Grunau, G.L,
Harris, A., Buckley, J., Todd, N.J., 2018. Diagnosis of ovarian torsion: is it
time to forget about doppler? J Obstet Gynaecol Can, 40, 871–875.
[12]. White, M., Stella,
J., 2005. Ovarian torsion: 10-year perspective. Emergency Medicine Australasia,
17, 231–237.
[13]. Oltmann, S.C.,
Fischer, A., Barber, R., Huang, R., Hicks, B., Garcia, N., 2009. Cannot exclude
torsion-a 15-year review. Journal of Pediatric Surgery, 44, 1212–1217.
[14]. Budhram, G., Elia,
T., Dan, J., Schroeder, M., Safain, G., Schlech, W., et al., 2019. A
Case-Control Study of Sonographic Maximum Ovarian Diameter as a Predictor of
Ovarian Torsion in Emergency Department Females with Pelvic Pain. Acad Emerg
Med, 26, 152–159.
[15]. Huchon, C.,
Fauconnier, A., 2010. Adnexal torsion: a literature review. European Journal
of Obstetrics and Gynecology and Reproductive Biology, 150, 8–12.
[16]. Descargues, G.,
Tinlot-Mauger, F., Gravier, A., Lemoine, J.P., Marpeau, L., 2001. Adnexal
torsion: a report on forty-five cases. Eur J Obstet Gynecol Reprod Biol,
98, 91–96.
[17]. Aishwarya, R.,
Ethirajan, S., 2022. Gestational age at booking for antenatal care in a
tertiary healthcare facility: a glance. International Journal of Infertility
& Fetal Medicine, 13(3), 91-95.
[18]. Omani-Samani, R.,
Hollins Martin, C. J., Martin, C. R., Maroufizadeh, S., Ghaheri, A., Navid, B.,
2021. The birth satisfaction scale-revised Indicator (BSS-RI): a validation
study in Iranian mothers. The Journal of Maternal-Fetal & Neonatal
Medicine, 34(11), 1827-1831.
[19]. Sandeep, S.,
Shanthi, E., 2020. Study on impact of maternal age on pregnancy outcome at a
tertiary care hospital. International Journal of Research in Pharmaceutical
Sciences, 11(2), 235-238.
[20]. Kirubamani, N. H.,
2014. Does Tubal Sterilization offer a Permanent Solution? Indian Journal of
Science and Technology, 7(4), 418.
